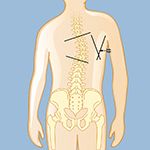
The degree of curvature is measured by drawing lines at the first and last tilted vertebrae, then drawing lines perpendicular to those lines. Where that second set of lines intersect, called the Cobb angle, is where the degree of the curve is measured.
Spinal deformities can often be clearly visible. However, to establish the extent of a spinal deformity and its cause, a neurosurgeon or orthopedic physician will begin by getting a complete medical history, including viewing any prior X-rays. The physician will look for asymmetries (uneven appearances) as a person sits, stands, and walks, paying special attention to the shoulders, ribs, chest, leg length, and other unusual findings, such as if the torso doesn’t appear to be evenly positioned over the pelvis, or a person’s head seems off-center. Current physical findings and measurements will be compared to prior records.
Other information will be gathered as well, including:
- Changes in a person’s height
- Family history, since some types of spinal deformities tend to run in families
- If there is bowel or bladder dysfunction, which may indicate nerve damage
- Onset of symptoms, or when spinal deformity was first noticed
- Pain, what intensifies it, and if any pain radiates from the spine itself, as well as tingling, numbness, impaired reflexes, and muscle weakness, indicating compression of nerves
- Past surgeries, as spinal deformities can be a result of previous back surgeries. Iatrogenic scoliosis (caused by prior medical treatment) often requires a second, revision surgery to correct. Examples include a spinal fusion that did not heal properly in a patient whose ligaments are not strong enough to support the spine, which causes the vertebrae to collapse.
Spinal deformities can be visualized with X-rays.
- X-rays from different angles can check for changes from past X-rays and determine progression of the curve or visualize any other bony abnormalities, fractures, and disc issues.
- Front-view full-length X-rays of the spinal column are taken as the individual stands with arms extended forward while keeping the head erect.
- Lateral-bend X-rays may be taken from the side while an individual is standing or bending sideways or backwards to see wedging of the vertebrae and determine flexibility.
Other tests may be ordered to diagnosis adult scoliosis and determine its severity and cause.
- Computerized tomography (CT) is a noninvasive procedure that uses X-rays to produce a three-dimensional image of the spine. A CT shows more details than an X-ray and can show the nerves, spinal cord, and any possible damage to them.
- Electromyogram and nerve-conduction studies (EMG/NCS) measure the electrical activity in the nerves and muscles. They may identify nerve damage or nerve compression.
- Magnetic resonance imaging (MRI) uses magnetic fields and radio-frequency waves to create an image of the spine that reveals the discs, nerves, spinal canal, and other details that can’t normally be seen on an X-ray. An MRI may also check for spinal-cord compression, as in spinal stenosis. Sometimes a contrast agent is injected into a vein in the hand or arm during the test, which highlights certain tissues and structures to make details even clearer.
- Myelograms involve a dye that is injected directly into the spinal column and are used in conjunction with CT scans.
- Pulmonary-function tests may be ordered to determine if lung function is restricted due to decreased space in the chest from the scoliosis.










